The Best Way To Address Fallen Arches
Overview

Rigid fallen arches are usually easy to distinguish from the flexible variety by the pain the cause, but there is a simple test that a person can perform if he is not sure. He should stand on the toes, and if the arch appears, the condition is known as flexible flat foot and is nothing to worry about. There have been Olympic runners with flat feet of this kind. On the other hand, if the foot remains flat on the bottom when the person stands on his toes, the condition is rigid, and the individual should consult a podiatrist. The same is true if a person notices any change in the arches of his feet or if he as foot pain, whether or not this test suggests he has flexible flat feet.
Causes
Most cases of flatfeet are simply the result of normal development. When that is not the case, the condition can be caused by a number of factors, including the following, Age, disease, injury, obesity or being overweight, physical abnormality, pregnancy. Flattened arches in adults may result from the stresses of aging, weight gain, and the temporary increase in elastin (protein in connective tissue) due to pregnancy. In some cases, flatfeet are caused by a physical abnormality, such as tarsal coalition (two or more bones in the foot that have grown together) or accessory navicular (an extra bone along the side of the foot). The effects of diseases such as diabetes and rheumatoid arthritis can lead to flatfeet. An injury (e.g., bone fracture, dislocation, sprain or tear in any of the tendons and ligaments in the foot and leg) also can cause flatfeet.
Symptoms
Pain and stiffness of the medial arch or anywhere along the mid-portion of the foot. Associated discomfort within and near the ankle joint. The knees, hips, and lower back may be the primary source of discomfort. Feet may often feel tired and achy. Painful shin splints may develop with activity. Gait may be awkward.
Diagnosis
You can test yourself to see if you have flat feet or fallen arches by using a simple home experiment. First, dip your feet in water. Then step on a hard flat surface, like a dry floor or a piece of paper on the floor, where your footprints will show. Step away and examine your foot prints. If you see complete/full imprints of your feet on the floor, you may have fallen arches. However, it?s important to seek a second option from a podiatrist if you suspect you have fallen arches so they can properly diagnose and treat you.
high arch feet
Non Surgical Treatment
If you have flat feet and foot pain, especially if one foot is flatter than the other, you should have an evaluation by an orthopedic surgeon . You may have a problem with the posterior tibial tendon , the main tendon that supports the arch. Factors that can contribute to this problem are obesity, diabetes , high blood pressure , certain types of arthritis and athletic overuse. In some cases a shoe insert/orthotic can be used to alleviate the symptoms of flat feet.
Surgical Treatment
In cases of flat feet that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required and in some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Rigid fallen arches are usually easy to distinguish from the flexible variety by the pain the cause, but there is a simple test that a person can perform if he is not sure. He should stand on the toes, and if the arch appears, the condition is known as flexible flat foot and is nothing to worry about. There have been Olympic runners with flat feet of this kind. On the other hand, if the foot remains flat on the bottom when the person stands on his toes, the condition is rigid, and the individual should consult a podiatrist. The same is true if a person notices any change in the arches of his feet or if he as foot pain, whether or not this test suggests he has flexible flat feet.
Causes
Most cases of flatfeet are simply the result of normal development. When that is not the case, the condition can be caused by a number of factors, including the following, Age, disease, injury, obesity or being overweight, physical abnormality, pregnancy. Flattened arches in adults may result from the stresses of aging, weight gain, and the temporary increase in elastin (protein in connective tissue) due to pregnancy. In some cases, flatfeet are caused by a physical abnormality, such as tarsal coalition (two or more bones in the foot that have grown together) or accessory navicular (an extra bone along the side of the foot). The effects of diseases such as diabetes and rheumatoid arthritis can lead to flatfeet. An injury (e.g., bone fracture, dislocation, sprain or tear in any of the tendons and ligaments in the foot and leg) also can cause flatfeet.
Symptoms
Pain and stiffness of the medial arch or anywhere along the mid-portion of the foot. Associated discomfort within and near the ankle joint. The knees, hips, and lower back may be the primary source of discomfort. Feet may often feel tired and achy. Painful shin splints may develop with activity. Gait may be awkward.
Diagnosis
You can test yourself to see if you have flat feet or fallen arches by using a simple home experiment. First, dip your feet in water. Then step on a hard flat surface, like a dry floor or a piece of paper on the floor, where your footprints will show. Step away and examine your foot prints. If you see complete/full imprints of your feet on the floor, you may have fallen arches. However, it?s important to seek a second option from a podiatrist if you suspect you have fallen arches so they can properly diagnose and treat you.
high arch feet
Non Surgical Treatment
If you have flat feet and foot pain, especially if one foot is flatter than the other, you should have an evaluation by an orthopedic surgeon . You may have a problem with the posterior tibial tendon , the main tendon that supports the arch. Factors that can contribute to this problem are obesity, diabetes , high blood pressure , certain types of arthritis and athletic overuse. In some cases a shoe insert/orthotic can be used to alleviate the symptoms of flat feet.
Surgical Treatment
In cases of flat feet that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required and in some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Do You Understand Heel Pain?
Overview

Heel pain is usually focused on the underside or the back of your heel. If your pain is on the underside of your heel, its likely cause is plantar fasciitis. Pain on the back of your heel, where the Achilles tendon attaches to the heel bone, is Achilles tendinitis. Although heel pain is rarely a symptom of a serious condition, it can interfere with your normal activities, particularly exercise.
Causes
The most common cause of heel pain is plantar fasciitis. Plantar fasciitis is a stretching of the plantar fascia, a ligament that runs from the ball of foot through the arch and is attached to the heel. It is that attachment which becomes aggravated and typically causes pain after being on your feet for lengths of time. Abnormal motion of the foot (pronation) is one cause of plantar fasciitis. Heel spurs, which are abnormal bone growths coming off the heel, can also cause heel pain. Other causes include repetitive stress or shock to the heel, standing for prolonged periods or osteoarthritis.
Symptoms
Initially, this pain may only be present when first standing up after sleeping or sitting. As you walk around, the muscle and tendon loosen and the pain goes away. As this problem progresses, the pain can be present with all standing and walking. You may notice a knot or bump on the back of the heel. Swelling may develop. In some cases, pressure from the back of the shoe causes pain.
Diagnosis
A biomechanical exam by your podiatrist will help reveal these abnormalities and in turn resolve the cause of plantar fasciitis. By addressing this cause, the patient can be offered a podiatric long-term solution to his problem.
Non Surgical Treatment
If you still have pain after several weeks, see your foot and ankle surgeon, who may add one or more of these treatment approaches, padding and strapping. Placing pads in the shoe softens the impact of walking. Strapping helps support the foot and reduce strain on the fascia. Orthotic devices. Custom orthotic devices that fit into your shoe help correct the underlying structural abnormalities causing the plantar fasciitis. Injection therapy. In some cases, corticosteroid injections are used to help reduce the inflammation and relieve pain. Removable walking cast. A removable walking cast may be used to keep your foot immobile for a few weeks to allow it to rest and heal. Night splint. Wearing a night splint allows you to maintain an extended stretch of the plantar fascia while sleeping. This may help reduce the morning pain experienced by some patients. Physical therapy. Exercises and other physical therapy measures may be used to help provide relief.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
deelsonheels
Prevention
Before you get out of bed in the morning, and then periodically throughout the day, do the following exercises to increase flexibility and ease pain. Slowly flex your foot and toes to stretch the tissue on the bottom of your sore foot. Hold the stretch for 10 counts. Relax and repeat. Do gentle ankle rolls to keep the tissues around the ankle and on the back of the heel flexible. Sit on the edge of your bed and roll your foot back and forth over a tennis ball.
Heel pain is usually focused on the underside or the back of your heel. If your pain is on the underside of your heel, its likely cause is plantar fasciitis. Pain on the back of your heel, where the Achilles tendon attaches to the heel bone, is Achilles tendinitis. Although heel pain is rarely a symptom of a serious condition, it can interfere with your normal activities, particularly exercise.
Causes
The most common cause of heel pain is plantar fasciitis. Plantar fasciitis is a stretching of the plantar fascia, a ligament that runs from the ball of foot through the arch and is attached to the heel. It is that attachment which becomes aggravated and typically causes pain after being on your feet for lengths of time. Abnormal motion of the foot (pronation) is one cause of plantar fasciitis. Heel spurs, which are abnormal bone growths coming off the heel, can also cause heel pain. Other causes include repetitive stress or shock to the heel, standing for prolonged periods or osteoarthritis.
Symptoms
Initially, this pain may only be present when first standing up after sleeping or sitting. As you walk around, the muscle and tendon loosen and the pain goes away. As this problem progresses, the pain can be present with all standing and walking. You may notice a knot or bump on the back of the heel. Swelling may develop. In some cases, pressure from the back of the shoe causes pain.
Diagnosis
A biomechanical exam by your podiatrist will help reveal these abnormalities and in turn resolve the cause of plantar fasciitis. By addressing this cause, the patient can be offered a podiatric long-term solution to his problem.
Non Surgical Treatment
If you still have pain after several weeks, see your foot and ankle surgeon, who may add one or more of these treatment approaches, padding and strapping. Placing pads in the shoe softens the impact of walking. Strapping helps support the foot and reduce strain on the fascia. Orthotic devices. Custom orthotic devices that fit into your shoe help correct the underlying structural abnormalities causing the plantar fasciitis. Injection therapy. In some cases, corticosteroid injections are used to help reduce the inflammation and relieve pain. Removable walking cast. A removable walking cast may be used to keep your foot immobile for a few weeks to allow it to rest and heal. Night splint. Wearing a night splint allows you to maintain an extended stretch of the plantar fascia while sleeping. This may help reduce the morning pain experienced by some patients. Physical therapy. Exercises and other physical therapy measures may be used to help provide relief.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
deelsonheels
Prevention
Before you get out of bed in the morning, and then periodically throughout the day, do the following exercises to increase flexibility and ease pain. Slowly flex your foot and toes to stretch the tissue on the bottom of your sore foot. Hold the stretch for 10 counts. Relax and repeat. Do gentle ankle rolls to keep the tissues around the ankle and on the back of the heel flexible. Sit on the edge of your bed and roll your foot back and forth over a tennis ball.
Functional Leg Length Discrepancy
Overview
Limb deformity or leg length problems can be treated by applying an external frame to the leg. The frame consists of metal rings which go round the limb. The rings are held onto the body by wires and metal pins which pass through the skin and are anchored into the bone. During this operation, the bone is divided. Gradual adjustment of the frame results in creation of a new bone allowing a limb to be lengthened. The procedure involves the child having an anaesthetic. The child is normally in hospital for one week. The child and family are encouraged to clean pin sites around the limb. The adjustments of the frame (distractions) are performed by the child and/or family. The child is normally encouraged to walk on the operated limb and to actively exercise the joints above and below the frame. The child is normally reviewed on a weekly basis in clinic to monitor the correction of the deformity. The frame normally remains in place for 3 months up to one year depending on the condition which is being treated. The frame is normally removed under a general anaesthetic at the end of treatment.
Causes
Some causes of leg length discrepancy (other than anatomical). Dysfunction of the hip joint itself leading to compensatory alterations by the joint and muscles that impact on the joint. Muscle mass itself, i.e., the vastus lateralis muscle, pushes the iliotibial band laterally, causing femoral compensations to maintain a line of progression during the gait cycle. This is often misdiagnosed as I-T band syndrome and subsequently treated incorrectly. The internal rotators of the lower limb are being chronically short or in a state of contracture. According to Cunningham's Manual of Practical Anatomy these are muscles whose insertion is lateral to the long axis of the femur. The external rotators of the hip joint are evidenced in the hip rotation test. The iliosacral joint displays joint fixations on the superior or inferior transverse, or the sagittal axes. This may result from many causes including joint, muscle, osseous or compensatory considerations. Short hamstring muscles, i.e., the long head of the biceps femoris muscle. In the closed kinetic chain an inability of the fibula to drop inferior will result in sacrotuberous ligament loading failure. The sacroiliac joint dysfunctions along its right or left oblique axis. Failure or incorrect loading of the Back Force Transmission System (the longitudinal-muscle-tendon-fascia sling and the oblique dorsal muscle-fascia-tendon sling). See the proceedings of the first and second Interdisciplinary World Congress on Low Back Pain. Sacral dysfunction (nutation or counternutation) on the respiratory axis. When we consider the above mentioned, and other causes, it should be obvious that unless we look at all of the causes of leg length discrepancy/asymmetry then we will most assuredly reach a diagnosis based on historical dogma or ritual rather than applying the rules of current differential diagnosis.
Symptoms
LLD do not have any pain or discomfort directly associated with the difference of one leg over the other leg. However, LLD will place stress on joints throughout the skeletal structure of the body and create discomfort as a byproduct of the LLD. Just as it is normal for your feet to vary slightly in size, a mild difference in leg length is normal, too. A more pronounced LLD, however, can create abnormalities when walking or running and adversely affect healthy balance and posture. Symptoms include a slight limp. Walking can even become stressful, requiring more effort and energy. Sometimes knee pain, hip pain and lower back pain develop. Foot mechanics are also affected causing a variety of complications in the foot, not the least, over pronating, metatarsalgia, bunions, hammer toes, instep pain, posterior tibial tendonitis, and many more.
Diagnosis
On standing examination one iliac crest may be higher/lower than the other. However a physiotherapist, osteopath or chiropractor will examine the LLD in prone or supine position and measure it, confirming the diagnosis of structural (or functional) LLD. The LLD should be measured using bony fixed points. X-Ray should be taken in a standing position. The osteopath, physiotherapist or chiropractor will look at femoral head & acetabulum, knee joints, ankle joints.
Non Surgical Treatment
In an adult, we find that we can add a non compressive silicone heel lift to a shoe in increments of 3-4 mm maximum per week. Were we to give a patient with a 20 mm short leg, 20 mm of lift all at once, their entire body would rebel. The various compensations that the body has made, such as curvatures and shortening of muscles on the convex side of the curve, would make such a dramatic change not just noticeable, but painful. When we get close to balancing a patient by lifting a leg with heel inserts, then we perform another gait analysis and follow up xray. At that point, we can typically write them a final prescription to have their shoe modified. A heel lift is typically fine up to 7 mm. When it gets higher than that, the entire shoe must be modified. There are two reasons for this. The back of the shoe is generally too short to accommodate more than 7-8 mm inserted inside the shoes and a heel lift greater than 7 mm will lead to Achilles tendon shortening, which then creates it?s own panoply of problems.

how to grow taller at 16
Surgical Treatment
For discrepancies over five centimeters, more aggressive surgical procedures-specifically leg lengthening procedures-are typically required. The specifics of this operative procedure are beyond the scope of this informational page, but your child's physician will be able to discuss the details in reference to your child's specific problems when considered appropriate.
Limb deformity or leg length problems can be treated by applying an external frame to the leg. The frame consists of metal rings which go round the limb. The rings are held onto the body by wires and metal pins which pass through the skin and are anchored into the bone. During this operation, the bone is divided. Gradual adjustment of the frame results in creation of a new bone allowing a limb to be lengthened. The procedure involves the child having an anaesthetic. The child is normally in hospital for one week. The child and family are encouraged to clean pin sites around the limb. The adjustments of the frame (distractions) are performed by the child and/or family. The child is normally encouraged to walk on the operated limb and to actively exercise the joints above and below the frame. The child is normally reviewed on a weekly basis in clinic to monitor the correction of the deformity. The frame normally remains in place for 3 months up to one year depending on the condition which is being treated. The frame is normally removed under a general anaesthetic at the end of treatment.
Causes
Some causes of leg length discrepancy (other than anatomical). Dysfunction of the hip joint itself leading to compensatory alterations by the joint and muscles that impact on the joint. Muscle mass itself, i.e., the vastus lateralis muscle, pushes the iliotibial band laterally, causing femoral compensations to maintain a line of progression during the gait cycle. This is often misdiagnosed as I-T band syndrome and subsequently treated incorrectly. The internal rotators of the lower limb are being chronically short or in a state of contracture. According to Cunningham's Manual of Practical Anatomy these are muscles whose insertion is lateral to the long axis of the femur. The external rotators of the hip joint are evidenced in the hip rotation test. The iliosacral joint displays joint fixations on the superior or inferior transverse, or the sagittal axes. This may result from many causes including joint, muscle, osseous or compensatory considerations. Short hamstring muscles, i.e., the long head of the biceps femoris muscle. In the closed kinetic chain an inability of the fibula to drop inferior will result in sacrotuberous ligament loading failure. The sacroiliac joint dysfunctions along its right or left oblique axis. Failure or incorrect loading of the Back Force Transmission System (the longitudinal-muscle-tendon-fascia sling and the oblique dorsal muscle-fascia-tendon sling). See the proceedings of the first and second Interdisciplinary World Congress on Low Back Pain. Sacral dysfunction (nutation or counternutation) on the respiratory axis. When we consider the above mentioned, and other causes, it should be obvious that unless we look at all of the causes of leg length discrepancy/asymmetry then we will most assuredly reach a diagnosis based on historical dogma or ritual rather than applying the rules of current differential diagnosis.
Symptoms
LLD do not have any pain or discomfort directly associated with the difference of one leg over the other leg. However, LLD will place stress on joints throughout the skeletal structure of the body and create discomfort as a byproduct of the LLD. Just as it is normal for your feet to vary slightly in size, a mild difference in leg length is normal, too. A more pronounced LLD, however, can create abnormalities when walking or running and adversely affect healthy balance and posture. Symptoms include a slight limp. Walking can even become stressful, requiring more effort and energy. Sometimes knee pain, hip pain and lower back pain develop. Foot mechanics are also affected causing a variety of complications in the foot, not the least, over pronating, metatarsalgia, bunions, hammer toes, instep pain, posterior tibial tendonitis, and many more.
Diagnosis
On standing examination one iliac crest may be higher/lower than the other. However a physiotherapist, osteopath or chiropractor will examine the LLD in prone or supine position and measure it, confirming the diagnosis of structural (or functional) LLD. The LLD should be measured using bony fixed points. X-Ray should be taken in a standing position. The osteopath, physiotherapist or chiropractor will look at femoral head & acetabulum, knee joints, ankle joints.
Non Surgical Treatment
In an adult, we find that we can add a non compressive silicone heel lift to a shoe in increments of 3-4 mm maximum per week. Were we to give a patient with a 20 mm short leg, 20 mm of lift all at once, their entire body would rebel. The various compensations that the body has made, such as curvatures and shortening of muscles on the convex side of the curve, would make such a dramatic change not just noticeable, but painful. When we get close to balancing a patient by lifting a leg with heel inserts, then we perform another gait analysis and follow up xray. At that point, we can typically write them a final prescription to have their shoe modified. A heel lift is typically fine up to 7 mm. When it gets higher than that, the entire shoe must be modified. There are two reasons for this. The back of the shoe is generally too short to accommodate more than 7-8 mm inserted inside the shoes and a heel lift greater than 7 mm will lead to Achilles tendon shortening, which then creates it?s own panoply of problems.
how to grow taller at 16
Surgical Treatment
For discrepancies over five centimeters, more aggressive surgical procedures-specifically leg lengthening procedures-are typically required. The specifics of this operative procedure are beyond the scope of this informational page, but your child's physician will be able to discuss the details in reference to your child's specific problems when considered appropriate.
Mortons Neuroma Solution
Overview
 Some sources claim that entrapment of the plantar nerve because of compression between the metatarsal heads, as originally proposed by Morton, is highly unlikely, because the plantar nerve is on the plantar side of the transverse metatarsal ligament and thus does not come in contact with the metatarsal heads. It is more likely that the transverse metatarsal ligament is the cause of the entrapment. Despite the name, the condition was first correctly described by a chiropodist named Durlacher, and although it is labeled a "neuroma", many sources do not consider it a true tumor, but rather a perineural fibroma (fibrous tissue formation around nerve tissue).
Some sources claim that entrapment of the plantar nerve because of compression between the metatarsal heads, as originally proposed by Morton, is highly unlikely, because the plantar nerve is on the plantar side of the transverse metatarsal ligament and thus does not come in contact with the metatarsal heads. It is more likely that the transverse metatarsal ligament is the cause of the entrapment. Despite the name, the condition was first correctly described by a chiropodist named Durlacher, and although it is labeled a "neuroma", many sources do not consider it a true tumor, but rather a perineural fibroma (fibrous tissue formation around nerve tissue).
Causes
Some say that this condition should not be called Morton's neuroma as, in fact, it is not actually a neuroma. A neuroma is a non-cancerous (benign) tumour that grows from the fibrous coverings of a nerve. There is no tumour formation in Morton's neuroma. The anatomy of the bones of the foot is also thought to contribute to the development of Morton's neuroma. For example, the space between the long bones (metatarsals) in the foot is narrower between the second and third, and between the third and fourth metatarsals. This means that the nerves that run between these metatarsals are more likely to be compressed and irritated. Wearing narrow shoes can make this compression worse.
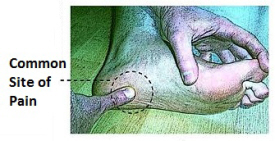
Symptoms
Normally, there are no outward signs, such as a lump, because this is not really a tumor. Burning pain in the ball of the foot that may radiate into the toes. The pain generally intensifies with activity or wearing shoes. Night pain is rare. There may also be numbness in the toes, or an unpleasant feeling in the toes. Runners may feel pain as they push off from the starting block. High-heeled shoes, which put the foot in a similar position to the push-off, can also aggravate the condition. Tight, narrow shoes also aggravate this condition by compressing the toe bones and pinching the nerve.
Diagnosis
To arrive at a diagnosis, the foot and ankle surgeon will obtain a thorough history of your symptoms and examine your foot. During the physical examination, the doctor attempts to reproduce your symptoms by manipulating your foot. Other tests or imaging studies may be performed. The best time to see your foot and ankle surgeon is early in the development of symptoms. Early diagnosis of a Morton?s neuroma greatly lessens the need for more invasive treatments and may avoid surgery.
Non Surgical Treatment
Initial therapies are nonsurgical and relatively simple. They can involve one or more of the following treatments. Changes in footwear. Avoid high heels or tight shoes, and wear wider shoes with lower heels and a soft sole. This enables the bones to spread out and may reduce pressure on the nerve, giving it time to heal. Orthoses. Custom shoe inserts and pads also help relieve irritation by lifting and separating the bones, reducing the pressure on the nerve. Injection. One or more injections of a corticosteroid medication can reduce the swelling and inflammation of the nerve, bringing some relief. Several studies have shown that a combination of roomier, more comfortable shoes, nonsteroidal anti-inflammatory medication, custom foot orthoses and cortisone injections provide relief in over 80 percent of people with Morton's Neuroma.
Surgical Treatment
When conservative measures are unsuccessful, surgery can be a good choice in the treatment of Morton's neuroma. The operation for Morton's neuroma does not require an overnight hospital stay. The anesthetic used is an ankle block, which completely numbs the foot during the surgery. The physician removes the neuroma from an incision made on the top of the foot between the involved metatarsal heads. The nerve to the interspace is exposed and cut next to the metatarsal heads.
Some sources claim that entrapment of the plantar nerve because of compression between the metatarsal heads, as originally proposed by Morton, is highly unlikely, because the plantar nerve is on the plantar side of the transverse metatarsal ligament and thus does not come in contact with the metatarsal heads. It is more likely that the transverse metatarsal ligament is the cause of the entrapment. Despite the name, the condition was first correctly described by a chiropodist named Durlacher, and although it is labeled a "neuroma", many sources do not consider it a true tumor, but rather a perineural fibroma (fibrous tissue formation around nerve tissue).Causes
Some say that this condition should not be called Morton's neuroma as, in fact, it is not actually a neuroma. A neuroma is a non-cancerous (benign) tumour that grows from the fibrous coverings of a nerve. There is no tumour formation in Morton's neuroma. The anatomy of the bones of the foot is also thought to contribute to the development of Morton's neuroma. For example, the space between the long bones (metatarsals) in the foot is narrower between the second and third, and between the third and fourth metatarsals. This means that the nerves that run between these metatarsals are more likely to be compressed and irritated. Wearing narrow shoes can make this compression worse.
Symptoms
Normally, there are no outward signs, such as a lump, because this is not really a tumor. Burning pain in the ball of the foot that may radiate into the toes. The pain generally intensifies with activity or wearing shoes. Night pain is rare. There may also be numbness in the toes, or an unpleasant feeling in the toes. Runners may feel pain as they push off from the starting block. High-heeled shoes, which put the foot in a similar position to the push-off, can also aggravate the condition. Tight, narrow shoes also aggravate this condition by compressing the toe bones and pinching the nerve.
Diagnosis
To arrive at a diagnosis, the foot and ankle surgeon will obtain a thorough history of your symptoms and examine your foot. During the physical examination, the doctor attempts to reproduce your symptoms by manipulating your foot. Other tests or imaging studies may be performed. The best time to see your foot and ankle surgeon is early in the development of symptoms. Early diagnosis of a Morton?s neuroma greatly lessens the need for more invasive treatments and may avoid surgery.
Non Surgical Treatment
Initial therapies are nonsurgical and relatively simple. They can involve one or more of the following treatments. Changes in footwear. Avoid high heels or tight shoes, and wear wider shoes with lower heels and a soft sole. This enables the bones to spread out and may reduce pressure on the nerve, giving it time to heal. Orthoses. Custom shoe inserts and pads also help relieve irritation by lifting and separating the bones, reducing the pressure on the nerve. Injection. One or more injections of a corticosteroid medication can reduce the swelling and inflammation of the nerve, bringing some relief. Several studies have shown that a combination of roomier, more comfortable shoes, nonsteroidal anti-inflammatory medication, custom foot orthoses and cortisone injections provide relief in over 80 percent of people with Morton's Neuroma.
Surgical Treatment
When conservative measures are unsuccessful, surgery can be a good choice in the treatment of Morton's neuroma. The operation for Morton's neuroma does not require an overnight hospital stay. The anesthetic used is an ankle block, which completely numbs the foot during the surgery. The physician removes the neuroma from an incision made on the top of the foot between the involved metatarsal heads. The nerve to the interspace is exposed and cut next to the metatarsal heads.
Shoe Lifts For Leg Length Discrepancy
There are two unique variations of leg length discrepancies, congenital and acquired. Congenital means that you are born with it. One leg is structurally shorter in comparison to the other. Through developmental periods of aging, the brain senses the gait pattern and recognizes some difference. The human body usually adapts by tilting one shoulder over to the "short" side. A difference of under a quarter inch isn't grossly excessive, demand Shoe Lifts to compensate and typically won't have a profound effect over a lifetime.

Leg length inequality goes mainly undiagnosed on a daily basis, yet this problem is very easily remedied, and can eradicate many instances of upper back pain.
Treatment for leg length inequality typically involves Shoe Lifts. These are generally very reasonably priced, commonly costing less than twenty dollars, compared to a custom orthotic of $200 and up. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Chronic back pain is easily the most prevalent health problem impacting men and women today. Around 80 million people have problems with back pain at some point in their life. It is a problem which costs companies millions every year due to lost time and production. Fresh and better treatment solutions are constantly sought after in the hope of reducing the economic influence this condition causes.

People from all corners of the earth experience foot ache due to leg length discrepancy. In most of these cases Shoe Lifts might be of very helpful. The lifts are capable of relieving any discomfort and pain in the feet. Shoe Lifts are recommended by many certified orthopaedic physicians.
To be able to support the human body in a nicely balanced fashion, the feet have a vital role to play. In spite of that, it is often the most neglected region of the body. Many people have flat-feet which means there may be unequal force placed on the feet. This will cause other body parts like knees, ankles and backs to be affected too. Shoe Lifts guarantee that suitable posture and balance are restored.
Leg length inequality goes mainly undiagnosed on a daily basis, yet this problem is very easily remedied, and can eradicate many instances of upper back pain.
Treatment for leg length inequality typically involves Shoe Lifts. These are generally very reasonably priced, commonly costing less than twenty dollars, compared to a custom orthotic of $200 and up. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Chronic back pain is easily the most prevalent health problem impacting men and women today. Around 80 million people have problems with back pain at some point in their life. It is a problem which costs companies millions every year due to lost time and production. Fresh and better treatment solutions are constantly sought after in the hope of reducing the economic influence this condition causes.
People from all corners of the earth experience foot ache due to leg length discrepancy. In most of these cases Shoe Lifts might be of very helpful. The lifts are capable of relieving any discomfort and pain in the feet. Shoe Lifts are recommended by many certified orthopaedic physicians.
To be able to support the human body in a nicely balanced fashion, the feet have a vital role to play. In spite of that, it is often the most neglected region of the body. Many people have flat-feet which means there may be unequal force placed on the feet. This will cause other body parts like knees, ankles and backs to be affected too. Shoe Lifts guarantee that suitable posture and balance are restored.
Have I Got Posterior Calcaneal Spur

Overview
Heel Spurs are deposits of calcium in the heel area of the foot that are the typically the result of tension, abrasion and/or inflammation in the plantar fascia attachment to the heel. The heel spur itself is said not to be painful. The pain likely arises from the inflammation of the plantar fascia. The plantar fascia encapsulates muscles in the sole of the foot. It supports the arch of the foot by acting as a bowstring to connect the ball of the foot to the heel. Common causes of heel spurs include excessive load on the foot from obesity or a sudden increase in weight, a sudden increase in walking or sports activities.
Causes
Heel spurs are exacerbated by an movements that stretch, twist or impact the plantar ligaments. Running, jumping, standing or walking on hard surfaces with unsupportive shoes, walking barefoot in sand are all activities that can activate heel spurs and plantar fasciitis. Obesity is another factor that increases stress to the plantar ligaments.

Symptoms
Symptoms may be similar to those of plantar fasciitis and include pain and tenderness at the base of the heel, pain on weight bearing and in severe cases difficulty walking. The main diagnosis of a heel spur is made by X-ray where a bony growth on the heel can be seen. A heel spur can occur without any symptoms at all and the athlete would never know they have the bony growth on the heel. Likewise, Plantar fasciitis can occur without the bone growth present.
Diagnosis
Diagnosis of a heel spur can be done with an x-ray, which will be able to reveal the bony spur. Normally, it occurs where the plantar fascia connects to the heel bone. When the plantar fascia ligament is pulled excessively it begins to pull away from the heel bone. When this excessive pulling occurs, it causes the body to respond by depositing calcium in the injured area, resulting in the formation of the bone spur. The Plantar fascia ligament is a fibrous band of connective tissue running between the heel bone and the ball of the foot. This structure maintains the arch of the foot and distributes weight along the foot as we walk. However, due to the stress that this ligament must endure, it can easily become damaged which commonly occurs along with heel spurs.
Non Surgical Treatment
Heel pain may be associated with a heel spur, however the heel pain is usually due to plantar fasciitis, rather than a heel spur, so treatment is usually directed at the plantar fasciitis itself. Treatment usually involves application of ice to reduce pain and inflammation, special stretching exercises, and pain-relieving or anti-inflammatory medicines. Night splints or orthotics may be recommended. It may help to avoid the activities that aggravate pain, such as long walks and running. Surgery is very rarely recommended and only after other measures fail.
Surgical Treatment
Surgery is used a very small percentage of the time. It is usually considered after trying non-surgical treatments for at least a year. Plantar fascia release surgery is use to relax the plantar fascia. This surgery is commonly paired with tarsal tunnel release surgery. Surgery is successful for the majority of people.
Prevention
You can help prevent heel spur symptoms from returning by wearing the proper shoes. Customized orthotics and insoles can help relieve pressure. It is important to perform your exercises to help keep your foot stretched and relaxed.
What Is Posterior Calcaneal Spur

Overview
The heel spur (or calcaneal spur) is a nail-like growth of calcium around the ligaments and tendons of the foot where they attach to the heel bone. The spur grows from the bone and into the flesh of the foot. A heel spur results from an anatomical change of the calcaneus (heel bone). This involves the area of the heel and occasionally, another disability, such as arthritis. The heel bone forms one end of the two longitudinal arches of the foot. These arches are held together by ligaments and are activated by the muscles of the foot (some of which are attached beneath the arches and run from the front to the back of the foot). These muscles and ligaments, like the other supporting tissues of the body, are attached in two places. Many are attached at the heel bone. The body reacts to the stress at the heel bone by calcifying the soft tissue attachments and creating a spur.
Causes
The calcaneal spur is seen most often in persons over the age of 40. The condition can also be associated with osteoarthritis, rheumatoid arthritis, poor circulation of the blood and other degenerative diseases. Men and women are equally likely to have them.

Symptoms
More often than not, heel spurs have no signs or symptoms, and you don?t feel any pain. This is because heel spurs aren?t pointy or sharp pieces of bone, contrary to common belief. Heel spurs don?t cut tissue every time movement occurs; they?re actually deposits of calcium on bone set in place by the body?s normal bone-forming mechanisms. This means they?re smooth and flat, just like all other bones. Because there?s already tissue present at the site of a heel spur, sometimes that area and the surrounding tissue get inflamed, leading to a number of symptoms, such as chronic heel pain that occurs when jogging or walking.
Diagnosis
Your doctor will review your medical history and examine your foot. X-rays are used to identify the location and size of the heel spur.
Non Surgical Treatment
There are both conservative and surgical heel spur treatment options. Because the heel pain caused by heel spurs is symptomatic of inflammation, the first step is to ice the area in hopes to reduce the inflammation. The next step is to see our orthopedic specialist to prescribe an appropriate treatment plan. Some conservative treatment options might include Anti-inflammatory medications. Shoe orthotics. Shoe inserts. If conservative treatments are not working, surgery may be required to remove the heel spur. As in all cases of heel pain, it is important to see an orthopedic doctor who specializes in foot and ankle pain.
Surgical Treatment
Most studies indicate that 95% of those afflicted with heel spurs are able to relieve their heel pain with nonsurgical treatments. If you are one of the few people whose symptoms don?t improve with other treatments, your doctor may recommend plantar fascia release surgery. Plantar fascia release involves cutting part of the plantar fascia ligament in order to release the tension and relieve the inflammation of the ligament. Sometimes the bone spur is also removed, if there is a large spur (remember that the bone spur is rarely a cause of pain. Overall, the success rate of surgical release is 70 to 90 percent in patients with heel spurs. One should always be sure to understand all the risks associated with any surgery they are considering.